Ill in England? Your Location Can Determine If You Live or Die
The NHS at 75 is missing most of its own targets. See what health access looks like in your constituency, from ambulance delays to cancer care waits
It’s becoming an all too familiar story as England’s National Health Service, which turns 75 on Wednesday, buckles under the weight of underfunding and a years-long backlog of patients waiting for vital operations.
Brexit has compounded the problem, contributing to staff shortages, while Covid-19 and demographic pressures have exacerbated record levels of long-term sickness that are only set to get worse. The crumbling healthcare system will be a major challenge for whoever wins the next election, due by January 2025.
A first-of-its-kind analysis by Bloomberg News of NHS data underscores how deep the problems run at the publicly-funded health service — and how difficult they will be to fix. It also shows that location really matters to the health care you receive. In many cases, a person’s postcode can affect whether they live or die after they seek urgent medical attention.
The analysis assessed how quickly patients can access health care in each of England’s 533 constituencies — the British term for electoral districts — and found that nearly every single area is failing to meet even half of eight key indicators tracked by the government, from hospital bed availability to ambulance waiting times. A fifth are meeting none.
For most indicators, Bloomberg measured local data against “intermediate ambitions” set out in two recent NHS plans that were drafted since the pandemic to try to pull the health service out of its current crisis. When compared with longer-term standards, even fewer targets are being met.
On four of the eight indicators — ambulance handover delays, the length of time it takes to administer diagnostic tests, start cancer treatment or receive a referral — all but a handful of constituencies are failing to meet goals.
Ambulance handovers — the length of time it takes for a patient to be transferred from an emergency vehicle to a hospital — should take fewer than 30 minutes in 95% of cases, according to the intermediate ambitions. In most parts of the country, that’s only happening about three-quarters of the time. In some areas, more than 70% of handovers take longer.
Once patients get to A&E, the British term for the emergency room, they should be treated, transferred or discharged within four hours at least 76% of the time, according to the interim targets. In some areas, this is the case for fewer than 60% of patients. Often that’s because there’s nowhere to put them so ambulances end up lining up outside hospitals. The data show that the overnight bed occupancy rate is as high as 98% in some parts of the country, although the NHS is managing to meet its target ratio of 92% or lower in almost half of constituencies.
“We’re delayed getting to jobs because we’re queuing at hospital; we’re queuing at hospital because there are no beds in A&E; there are no beds in A&E because there are no beds anywhere else in the hospital,” said Gabby Bone, who is based in Bristol, the largest city in the South West of England, and has worked for the ambulance service for more than seven years. “There’s no one service that’s a problem — it’s everything.”
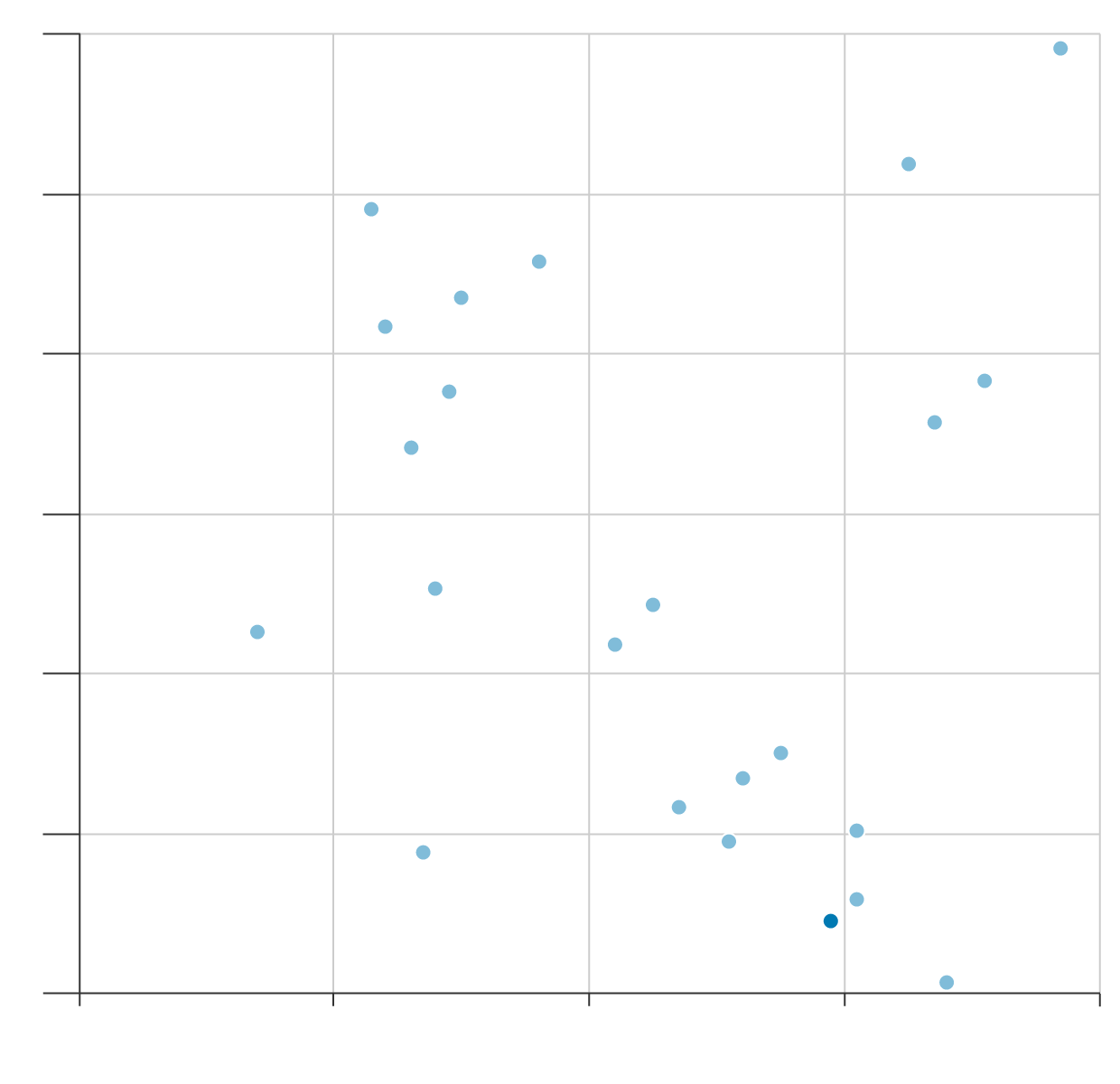
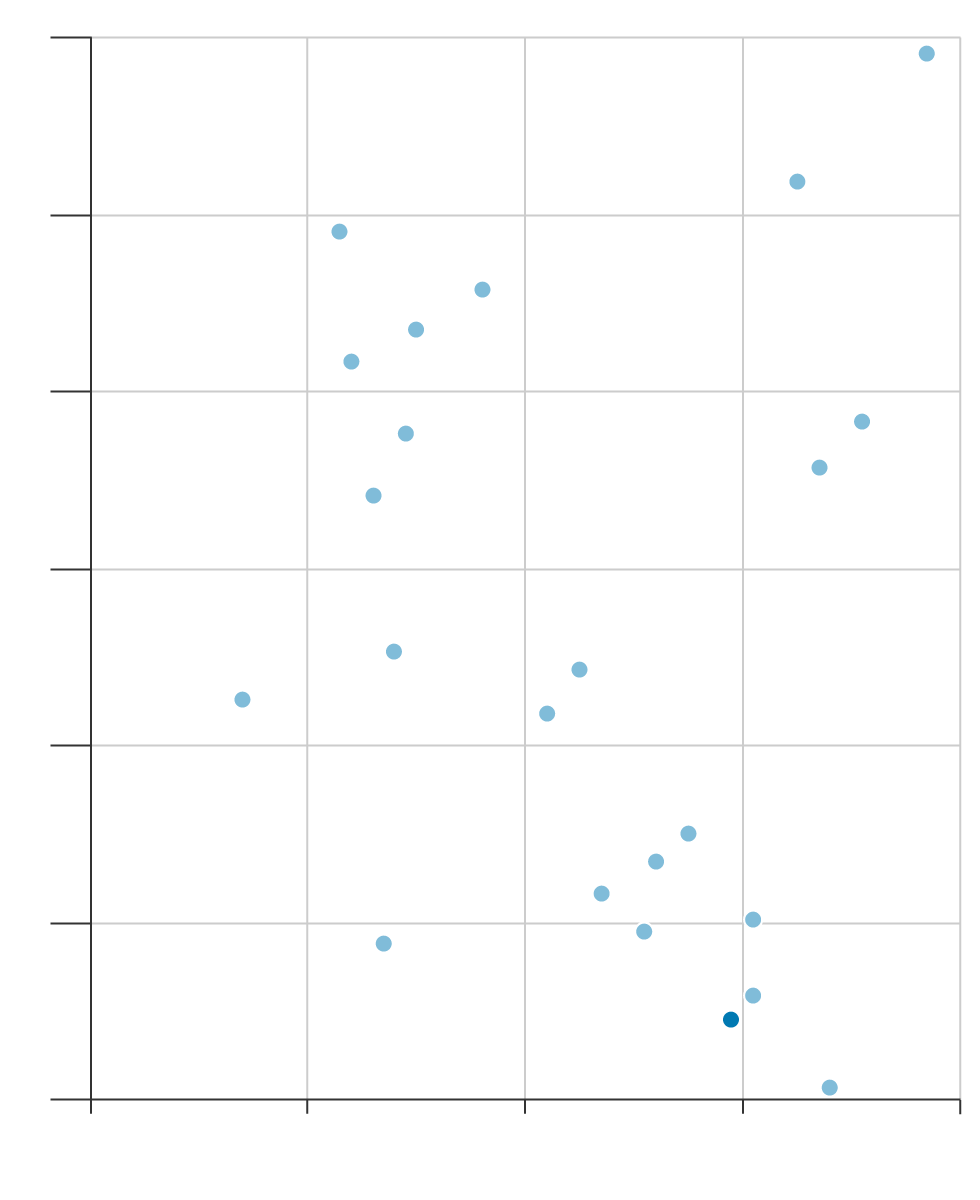
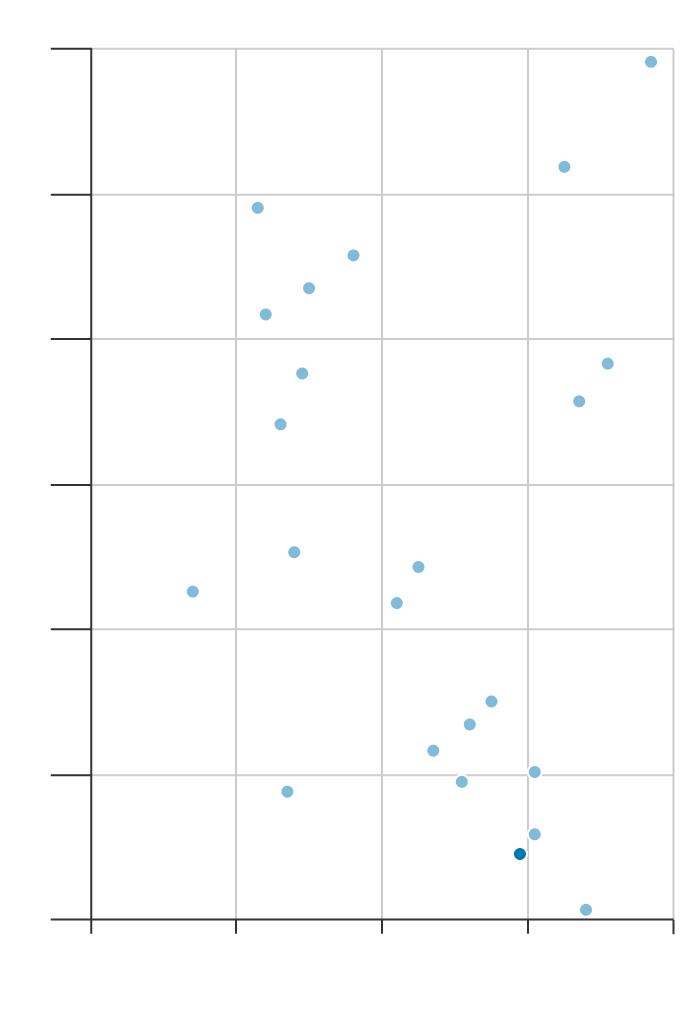
The total number of hospital beds in England has halved over the past 30 years, according to the King’s Fund, a health charity. While some of that may be attributable to an increase in same-day operations, the high occupancy rates also indicate a shortage. The UK has one of the lowest ratios of beds to population in Europe, despite being one of the bigger spenders on health care.
Spending More Doesn’t Guarantee a Bed
8
Germany
SPENT LESS,
MORE BEDS
SPENT MORE,
MORE BEDS
7
6
France
5
▶ Hospital beds per 1,000 population
4
Portugal
Italy
Netherlands
3
Spain
SPENT LESS,
FEWER BEDS
SPENT MORE,
FEWER BEDS
UK
Sweden
2
8
6
4
10
12
▶ Health spending as % of GDP
8
Germany
SPENT LESS,
MORE BEDS
SPENT MORE,
MORE BEDS
7
6
France
5
▶ Hospital beds per 1,000 population
4
Portugal
Italy
Netherlands
3
Spain
UK
SPENT LESS,
FEWER BEDS
SPENT MORE,
FEWER BEDS
Sweden
2
8
6
4
10
12
▶ Health spending as % of GDP
8
Germany
SPENT
MORE,
MORE
BEDS
7
6
France
5
▶ Hospital beds per 1,000 population
4
Portugal
Italy
Neth.
3
Spain
SPENT
LESS,
FEWER
BEDS
UK
Sweden
2
8
6
4
10
12
▶ Health spending as % of GDP
Diagnostic tests should be administered to at least 95% of patients within six weeks, according to the targets. On average, that’s only happening around 70% of the time and some constituencies aren’t even hitting 50%.
Wendy Davey, the 80-year-old stroke victim, didn’t know it as she waited for her ambulance to arrive, but her geographic location may have had a major impact on the care she received. North Somerset, her constituency, is among those meeting none of the metrics. Earlier this year, ambulance handovers were taking longer than 30 minutes in more than half of cases and nearly 27% of A&E patients in the area had to wait more than four hours to be processed. Take all the metrics together and the South West comes out as the worst performing region in England.

Living in an affluent area doesn’t necessarily guarantee good access to health care, according to the data. While London areas such as Kensington predictably rank high in Bloomberg’s analysis, constituencies in the wealthy South East trail the less prosperous North East, which is home to five of the top 20 performing constituencies. One major driver is population growth putting pressure on services. That could explain why Bristol is struggling: its population grew 10% to just under half a million people in the decade through 2021.
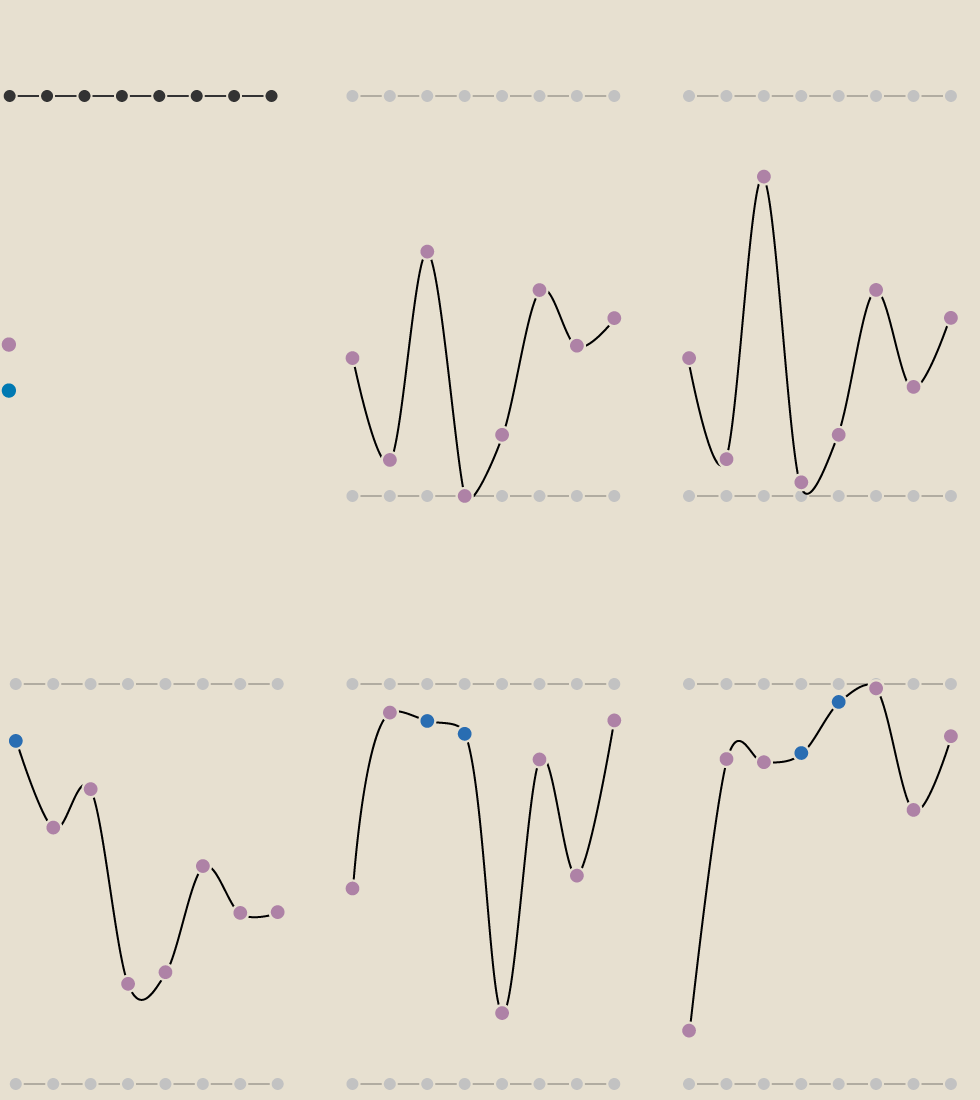
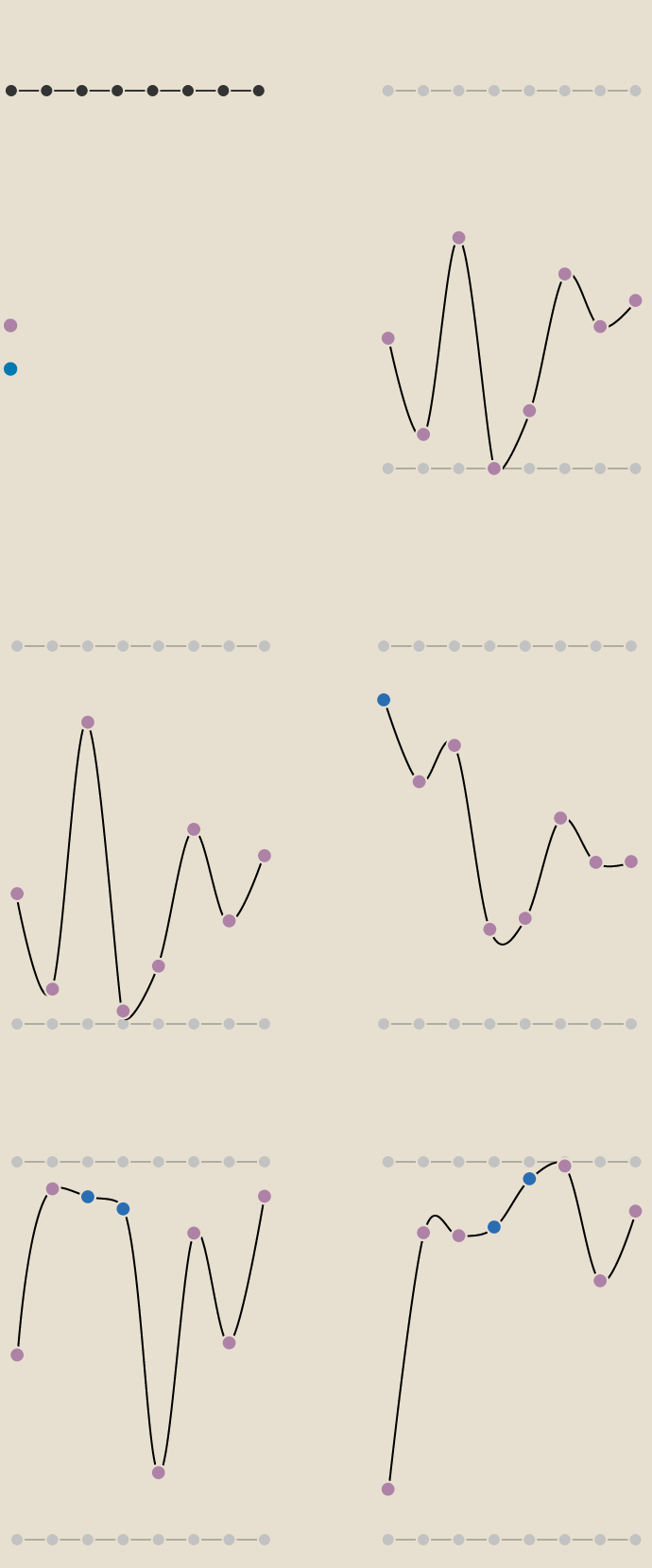
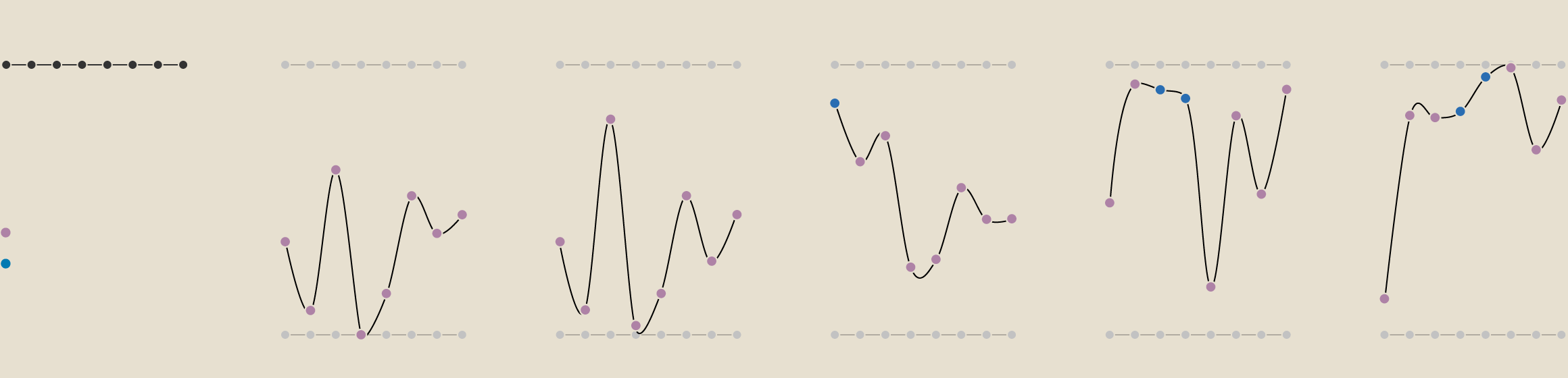
Postcode Lottery
Bristol
South
North
Somerset
AMBULANCE ARRIVAL
TREATMENT
GP
AMBULANCE HANDOVER
A&E
HOSPITAL BEDS
DIAGNOSTIC TEST
CANCER
Highest ranking
Behind target
Meeting or
exceeding target
Lowest ranking
Brighton,
Pavilion
Newcastle upon
Tyne Central
Kensington
Bristol
South
North
Somerset
AMBULANCE ARRIVAL
TREATMENT
GP
AMBULANCE HANDOVER
A&E
HOSPITAL BEDS
DIAGNOSTIC TEST
CANCER
Highest ranking
Behind target
Meeting or
exceeding target
Lowest ranking
Brighton,
Pavilion
Newcastle upon
Tyne Central
Kensington
Bristol
South
AMBULANCE ARRIVAL
TREATMENT
GP
AMBULANCE HANDOVER
A&E
HOSPITAL BEDS
DIAGNOSTIC TEST
CANCER
Highest ranking
Behind target
Meeting or
exceeding target
Lowest ranking
North
Somerset
Brighton,
Pavilion
Newcastle upon
Tyne Central
Kensington
Bristol
South
North
Somerset
Brighton,
Pavilion
Newcastle upon
Tyne Central
Kensington
AMBULANCE ARRIVAL
TREATMENT
GP
AMBULANCE HANDOVER
A&E
HOSPITAL BEDS
DIAGNOSTIC TEST
CANCER
Highest ranking
Behind target
Meeting or
exceeding target
Lowest ranking
Stroke victims are particularly vulnerable because millions of neurons in the brain die every minute a typical stroke goes untreated. While average ambulance response times in England for emergency calls like strokes have recently fallen to around 30 minutes, for much of 2022 they were closer to an hour, peaking at an average of one hour and 33 minutes last December, according to NHS data. Someone in the UK has a stroke roughly every five minutes, according to Stroke Association, a charity.
A major driver of regional disparities is variation in supply and demand in different parts of the country, according to Siva Anandaciva, chief analyst on the policy team at The King’s Fund. While London may have the best hospitals, rural areas often have a higher share of elderly patients.
Existential Crisis
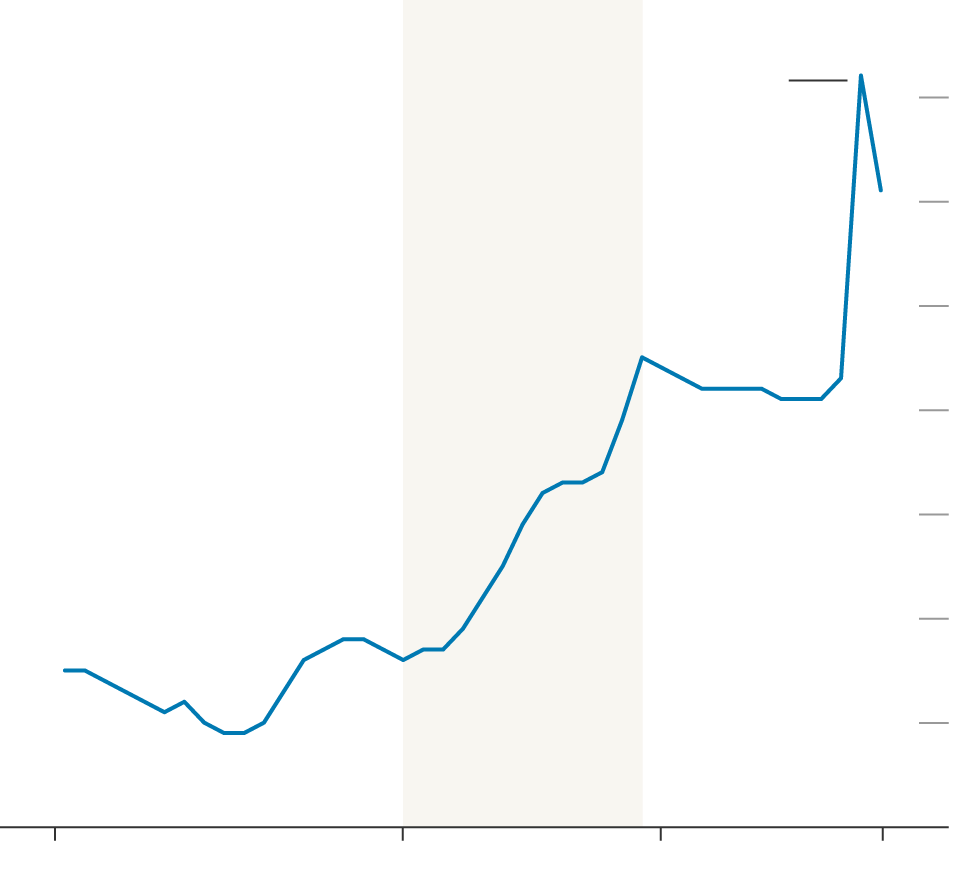
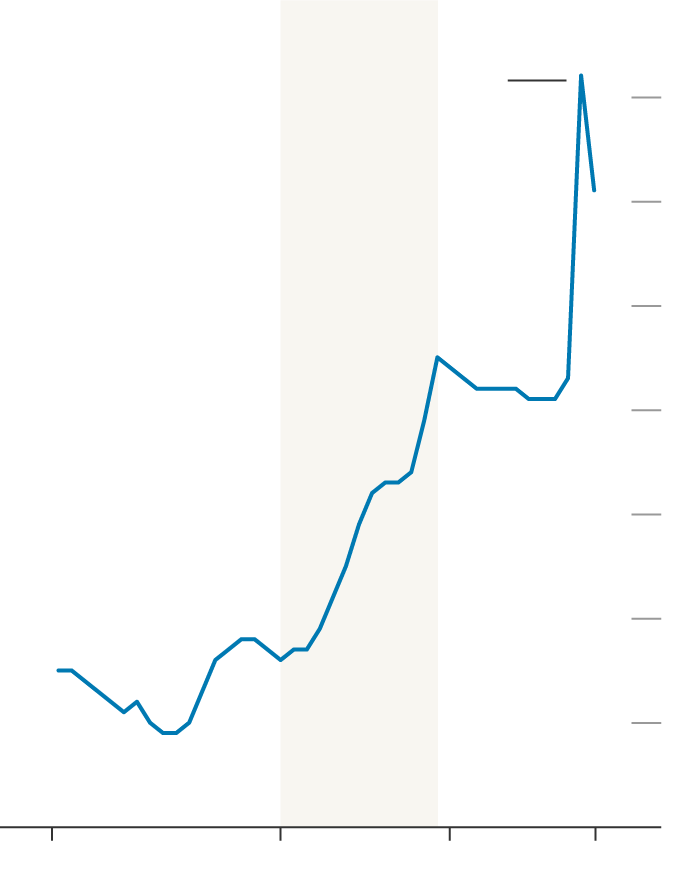
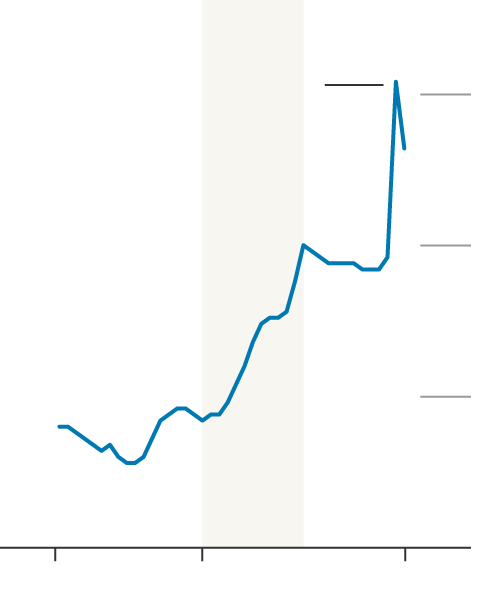
Public Sector Expenditure on Health
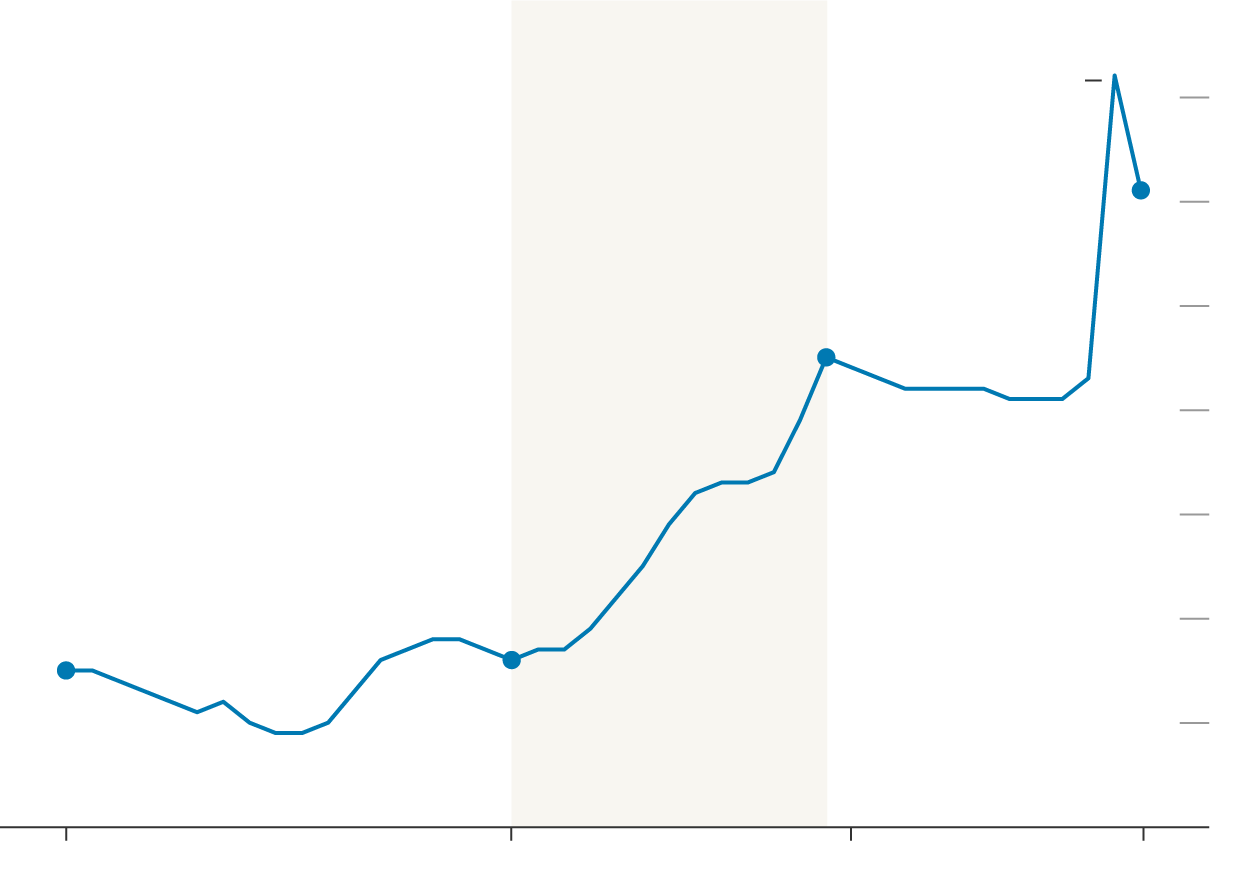
Conservative
Labour
Conservative
10%
Spending increased by
2.9 percentage points
during the Covid-19
pandemic
9
9.1%
8
7.5%
7
6
5
4.5%
4.6%
4
3
1980/81
1997/98
2010/11
2021/22
CONSERVATIVE
LABOUR
CONSERVATIVE
10%
Spending increased by
2.9 pct. pts during the
Covid-19 pandemic
9
8
7
6
5
4
3
1980/81
1997/98
2010/11
2021/22
CONSERVATIVE
LABOUR
CON.
10%
Spending increased by
2.9 pct. pts during the
Covid-19 pandemic
9
8
7
6
5
4
3
1980/81
1997/98
2010/11
2021/22
CONSERVATIVE
LABOUR
CON.
10.0%
Spending increased by
2.9 pct. pts during the
Covid-19 pandemic
7.5
5.0
2.5
1980/81
1997/98
2021/22
The data paint a picture of an institution that’s grappling with an existential crisis three quarters of a century after it was set up to provide free universal health care to everyone in the country. Brexit campaigners infamously promised that Britain’s exit from the European Union would free up more money for the health service. That didn’t happen and now many are questioning whether any amount of extra funding or reform will be enough to get the system back on its feet.
The problems were in place long before the pandemic due to failures to keep up with demand, reform and invest in technology, according to Karin Smyth, Labour MP for Bristol South and a shadow health minister. “The chickens have come home to roost,” she said.
While the emergency care crisis is the most visible, a harder problem to fix is the enormous backlog that’s holding up non-urgent procedures. As of April, 7.4 million people were waiting for treatment. This number could easily double to 14 million if everyone who’s held off treatment comes forward, according to an NHS estimate.
A major challenge keeping the NHS from untangling this web of delays is that Britain’s decision to leave the EU has exacerbated a staffing shortage just as demand has surged due to an aging population and an increase in long-term conditions. That situation is only set to get worse: the number of people older than 85 in England will double to 2.6 million over the next 25 years, according to a report published by the Health Foundation in 2021.
The crunch is putting more pressure on NHS staff, who are burned out and have effectively taken a pay cut over more than a decade due to inflation. The dispute has prompted strikes from junior doctors, nurses and ambulance staff, further straining the overall system. Many have left to work in countries like Australia and New Zealand, where conditions are more favorable, leaving more than 110,000 vacancies. The government predicts that number could grow to 360,000 by 2037 without action.

The government published a 15-year plan last week to recruit and retain NHS workers. Proposals, which aim to increase the pool of doctors by 60,000 by 2036-37, include placing trainees in practices and wards sooner and opening new medical schools in areas with the biggest staffing shortages. The opposition Labour Party, currently ahead in the polls, has pledged to cut ambulance waiting times, bring A&E turnarounds back to the four-hour target and decrease the inequality gap among regions.
“Cutting waiting times is one of the government’s top five priorities and we are making progress on our plans to recover and improve services,” a spokesperson for the Department of Health and Social Care said.
Many in the UK health sector say one way to relieve the pressure in the long term would be to improve services that can take the strain off hospitals. In theory, social care providers should be able to take responsibility for some patients with ongoing health conditions. These partially taxpayer-funded organizations can support people with illness, disability and elderly care, but pay in the sector is among the lowest in the country. The vacancy rate hit a record high last year, according to the workforce development and planning body Skills for Care.
The NHS needs to modernize and think about treating disease in a different way, said John Bell, regius professor of medicine at the University of Oxford and a long-standing adviser to the UK government. We have to invest more in identifying and tackling disease earlier if we want to “stop the hospitals from falling over and the GPs from being overwhelmed,” he said.
Signs of Improvement
The regional health data do show some signs of improvement over the past year as the NHS recovers from the pandemic. Ambulance response times and handover delays have shortened in more than 400 constituencies, while A&E waiting times are down in about half of England. Diagnostic test and referred treatment waiting times have also seen some progress.
But two indicators show broad deterioration: hospital bed occupancy, where nearly 500 constituencies have seen rates inch up over the past year; and GP waiting times, where nearly as many constituencies are failing to provide as many same- or next-day appointments as are needed.
It ultimately took Davey around two years from the time of her first stroke until she was connected with a GP who could see her regularly and promptly. Before that, she says she was sometimes waiting up to two months for an appointment while suffering bouts of searing pain in her left arm.
Her story also gives a hint of where the NHS might be headed. As the health service crumbles, record numbers of the public are choosing — or being forced — to pay for private services, and Davey is no exception. Some stroke survivors undergo physiotherapy in order to regain their mobility, but Davey quickly concluded that in order to be able to walk again, she would need to pay for private services which extended beyond what the NHS provided. She estimates she’s spent at least £9,000 ($11,500) since 2021 on physio and neurotherapy.
Total in-patient private admissions rose to 272,000 last year, an increase of 37% from pre-pandemic levels, according to the Private Healthcare Information Network. But the increase in patients willing to pay for health care doesn’t reduce pressure on the NHS because the private sector draws on the same pool of doctors and nurses, many of whom do some private work to supplement their pay. That in turn takes resources away from people who don’t have the means to pay for health care, while those who can pay for non-urgent treatment still rely on the NHS for emergency care anyway.
“If I had a stroke and I didn’t have any savings, I don’t know how I would have survived,” Davey said. “It would have been a case of just sitting in a chair with somebody coming in and washing me and getting me dressed. I would be just useless.”